Mary’s case revealed the Sequence Gap. Here is the clinical order FMU uses before the first protocol.
Dear Colleague and Friend,
Last week, I shared Mary’s case and invited you to pause before choosing the first clinical move.
Mary’s case was not meant to give you another protocol.
It was meant to reveal something deeper.
A complex patient can present with gut symptoms, blood sugar changes, thyroid concerns, inflammation, poor sleep, anxiety, pain,
and fatigue — and several of those findings may be real at the same time.
But the first clinical decision is still not obvious.
That is the Sequence Gap™.
The Sequence Gap appears when a clinician can identify many things that may be true, but does not yet have a clear clinical order for deciding what should happen first, what should wait, and what should change as the patient responds.
Today, I want to take the next step.
I do not want to simply tell you that sequencing matters.
I want to show you the clinical order FMU uses before choosing the first protocol, lab, supplement, or intervention.
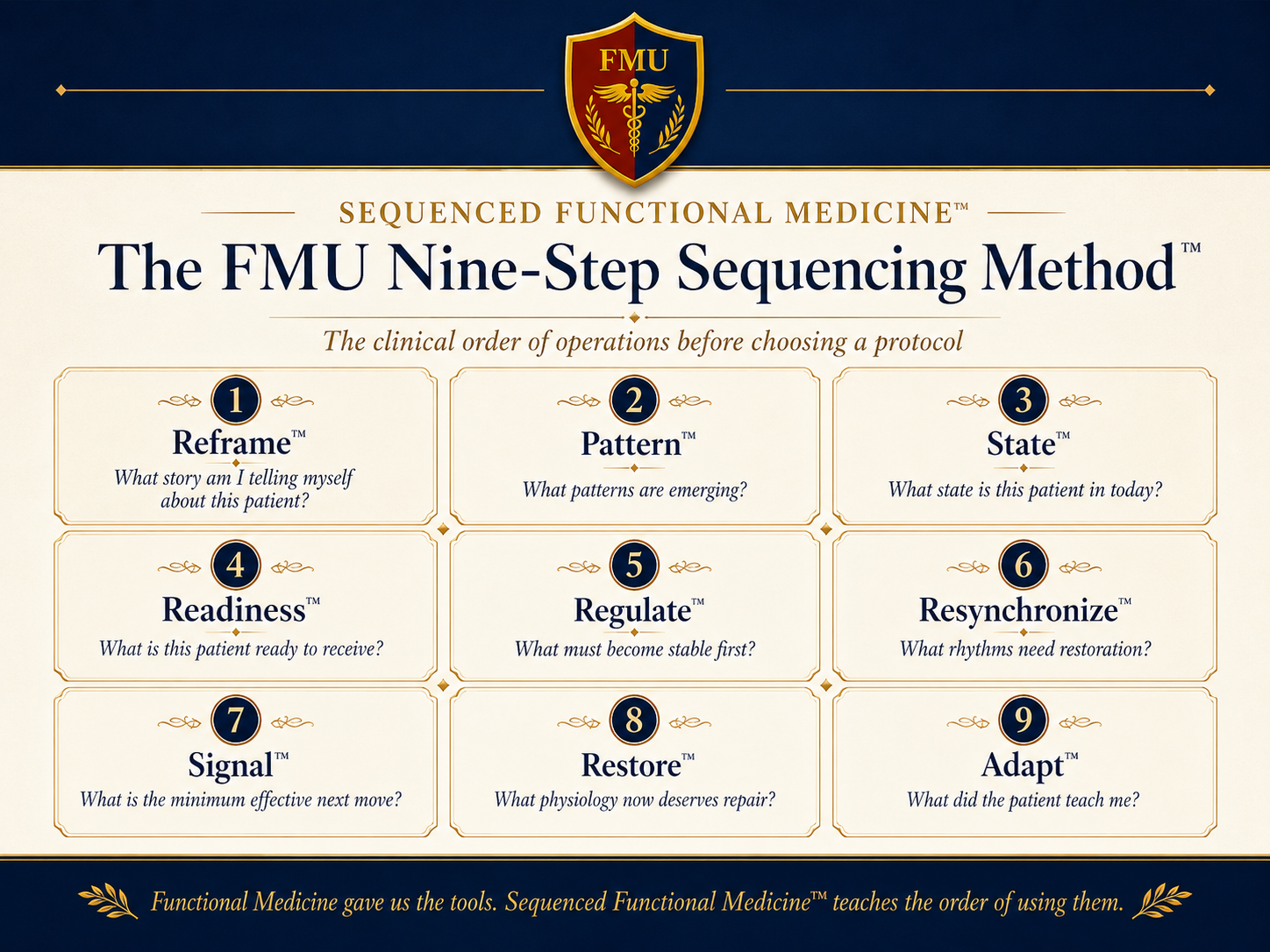
At FMU, we call this the FMU Nine-Step Sequencing Method™.
It is not a protocol.
It is not another clinical lane.
It is
a disciplined way to slow down, organize the case, and decide what deserves priority for the patient sitting in front of you.
The nine steps are:
1. Reframe™ — What story am I telling myself about this patient?
2. Pattern™— What patterns are emerging beneath the symptoms, history, and labs?
3.
State™— What state is this patient in today?
4. Readiness™ — What is this patient actually ready to receive?
5.
Regulate™— What must become more stable before deeper repair?
6. Resynchronize™— What biological rhythms need to be restored?
7. Signal™— What is the minimum effective next move?
8. Restore™ — Now that the patient has capacity, what physiology deserves repair?
9. Adapt™ — What did this patient teach me, and how should the plan change?
This sequence has become central to the way I think through complex cases.
And here is the important point:
Many clinicians do some of these steps.
But the clinical power comes from moving through the steps deliberately — and in the right
order.
Some experienced clinicians may read this and think, “Ron, I already sequence.”
I believe you. Every thoughtful clinician sequences to some degree. But the deeper question is not whether you sequence. The deeper question is: what
governs your sequence?
Is it the first abnormal lab, the loudest symptom, the protocol you know best, or the clinical lane where you have had the most success? Or is it a deliberate clinical order that moves the case from Reframe™ all the way to Adapt™?
One of the most common mistakes in complex Functional Medicine cases is jumping from Pattern™ directly to Restore™.
We see a gut pattern, so we begin restoring the gut.
We see a
hormone pattern, so we begin supporting hormones.
We see a lab abnormality, so we begin correcting the marker.
Those decisions may be reasonable.
But Mary’s case shows why they may still be too early.
If Mary is exhausted, sleeping poorly, reacting to supplements, struggling with anxiety, and feeling worse every time she starts something new, then the question is not simply, “Which protocol fits?”
The question becomes:
Did I move through the sequence before I chose the protocol?
Did I reframe the case?
Did I identify the larger pattern?
Did I understand her current state?
Did I assess readiness?
Did I regulate before trying to restore?
Did I choose the minimum effective next
signal?
Did I leave room to adapt based on her response?
That is where Sequenced Functional Medicine™ changes the conversation.
The goal is not to make
Functional Medicine more complicated.
The goal is to make complex cases more organized.
For the new Functional Medicine clinician, this sequence gives structure from the beginning so you do not drown in disconnected information.
For the experienced clinician, it provides a way to examine your clinical reflexes and ask whether your strongest lane has quietly begun to govern too many first decisions.
This is not about abandoning what you already know.
It is about organizing what you already know into a clearer clinical decision process.
Functional Medicine gave us the tools.
Sequenced Functional
Medicine™ teaches the clinical order of using them.
In my next message, I want to begin unpacking the first step:
Reframe™.
Because before we choose a protocol, before we order another test, and before we decide which clinical lane deserves attention, we have to ask a more fundamental question: what story am I already telling myself about this patient?
Before your next complex patient, ask yourself:
Which of these nine steps am I most likely to skip?
That single question may reveal where the Sequence Gap appears in your own clinical reasoning.
If this way of thinking resonates with you, this is the kind of clinical reasoning we teach inside FMU: comprehensive Functional Medicine, organized through a disciplined clinical order of operations.
Ronald Grisanti, D.C., D.A.B.C.O., D.A.C.B.N., M.S., DIANM, CFMP
P.S. The question is not whether you know Functional Medicine. The question is whether you are moving the case through a complete sequence before choosing what to do
first.
2123 Old Spartanburg Road #348 Greer South Carolina 29650 USA